
Non-Hodgkin Lymphoma Subtypes Among Indians and the Market Beyond 2026
Epidemiology, Biological Diversity, Therapeutic Transformation, and the Future Oncology Economy
Author Devanssh Mehta Mode
Introduction: Understanding India’s Emerging Lymphoma Landscape
Among the major hematological malignancies shaping modern oncology, Non-Hodgkin Lymphoma (NHL) occupies a unique and increasingly important position.
Unlike many solid tumors that arise from a single organ, NHL represents a biologically diverse family of cancers originating from lymphocytes—principally B cells, T cells, and natural killer (NK) cells. The disease spectrum ranges from indolent disorders with prolonged survival to highly aggressive malignancies demanding immediate intervention.
Globally, NHL has become one of the most dynamic oncology segments because of advances in:
- Molecular pathology
- Immunophenotyping
- Precision diagnostics
- Monoclonal antibodies
- Cellular immunotherapy
- Biomarker-driven treatment selection
In India, lymphoma presents an additional layer of complexity.
India’s epidemiological profile differs from Western populations due to:
- Younger demographic distribution
- Variable access to diagnosis
- Geographic heterogeneity
- Distinct infectious exposures
- Economic variability
- Rapid healthcare modernization
The coming decades beyond 2026 may therefore transform Indian lymphoma care from a predominantly treatment-centered model into a precision-driven, continuously monitored oncology ecosystem.
1. Non-Hodgkin Lymphoma: Biological Foundations
Non-Hodgkin lymphoma refers to malignant proliferation of lymphoid cells.
Broad classification:
B-cell lymphomas (~majority of Indian NHL burden)
Examples:
- Diffuse Large B-Cell Lymphoma (DLBCL)
- Follicular lymphoma
- Mantle cell lymphoma
- Marginal zone lymphoma
- Burkitt lymphoma
T-cell and NK-cell lymphomas
Examples:
- Peripheral T-cell lymphoma
- Anaplastic large cell lymphoma
- Extranodal NK/T-cell lymphoma
NHL develops through sequential alterations:
Normal lymphocyte
↓
Genetic instability
↓
Clonal expansion
↓
Immune escape
↓
Tumor evolution
Modern lymphoma science increasingly recognizes NHL as multiple diseases rather than a single diagnosis.
2. Epidemiology of NHL Among Indians



Lymphomas collectively constitute an important proportion of Indian cancers and represent one of the leading hematologic malignancies in the country.
Indian epidemiological observations suggest:
- Increasing diagnosed incidence
- Higher burden in urban regions
- Greater male predominance
- Significant regional variability
- Rising detection due to improved pathology access
Several factors contribute to apparent growth:
Demographic transition
Longer lifespan increases cancer prevalence.
Diagnostic expansion
Better pathology and imaging increase case detection.
Environmental changes
Urbanization and exposure shifts may influence risk.
Awareness growth
Earlier referral patterns improve recognition.
Importantly, increasing incidence does not necessarily imply worsening disease biology—it may also reflect better healthcare access.
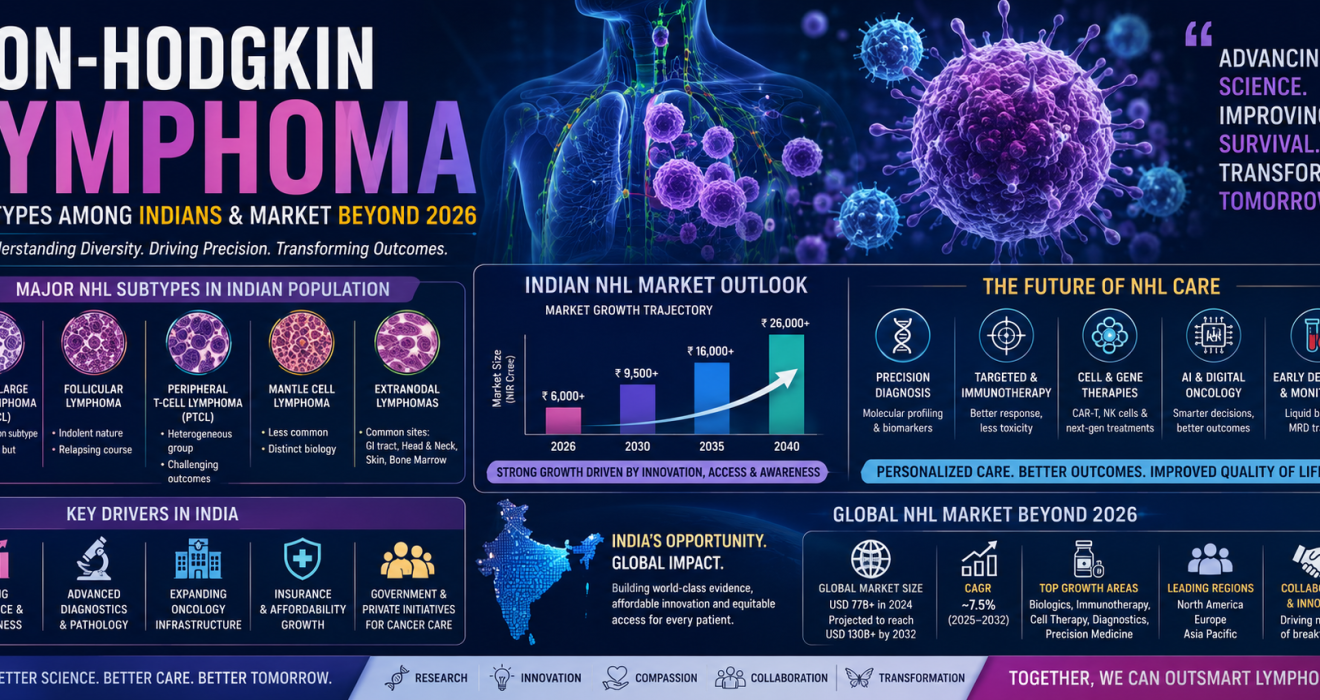
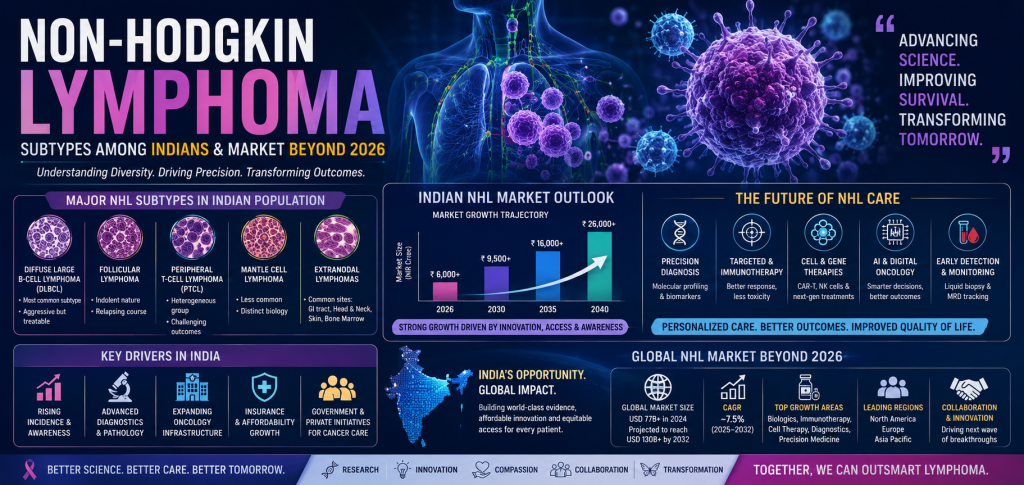
3. Distribution of NHL Subtypes in Indian Populations
India demonstrates a somewhat different subtype distribution compared with many Western countries.
A. Diffuse Large B-Cell Lymphoma (DLBCL)
The dominant subtype.
Estimated to account for the largest proportion of Indian NHL diagnoses.
Characteristics:
- Aggressive clinical behavior
- Rapid enlargement
- Extranodal presentation not uncommon
Typical molecular categories:
- Germinal center subtype
- Activated B-cell subtype
Future direction:
Precision stratification.
B. Follicular Lymphoma
Traditionally lower relative prevalence in India than Western populations.
Characteristics:
- Indolent behavior
- Relapsing course
- Long-term management focus
Growth outlook:
Increasing diagnosis due to improved pathology.
C. Mantle Cell Lymphoma
Relatively uncommon but clinically significant.
Features:
- Aggressive biology
- Older age predominance
- Emerging targeted treatment opportunities
D. Peripheral T-Cell Lymphoma (PTCL)
Clinically challenging subgroup.
Features:
- Biological heterogeneity
- Historically poorer outcomes
- Growing immunotherapy interest
E. Extranodal Lymphomas
Indian populations frequently report extranodal presentations.
Common sites:
- Gastrointestinal tract
- Head and neck
- Bone marrow
- Skin
Figure 1 — Illustrative Relative Distribution of Indian NHL Subtypes
| Subtype | Relative Contribution (Illustrative) |
|---|---|
| DLBCL | 40–50% |
| Follicular | 10–20% |
| PTCL | 10–15% |
| Mantle Cell | 5–10% |
| Others | Remaining |
Values are indicative synthesis for educational discussion and not a national registry estimate.
4. Why Indian NHL Looks Different
Indian lymphoma biology reflects interactions across:
Genetics
Population-level variation.
Infectious background
Immune signaling differences.
Delayed diagnosis
Advanced-stage presentation.
Resource variability
Diagnostic inconsistency.
Healthcare access
Treatment timing differences.
These variables create opportunities for India-specific oncology innovation.
5. Evolution of NHL Diagnosis Beyond 2026
Traditional diagnosis:
Histopathology.
Future diagnosis:
Integrated biological profiling.
Expected diagnostic stack:
Clinical assessment
- Imaging
- Immunophenotyping
- Molecular diagnostics
- AI support
- Longitudinal monitoring
Emerging technologies:
Digital pathology
AI-assisted morphology.
Liquid biopsy
Minimal residual disease detection.
Molecular sequencing
Treatment prediction.
Multi-omics oncology
Integrated biological analysis.
6. Therapeutic Evolution: From Chemotherapy to Precision Lymphoma Medicine
Historically:
CHOP-like chemotherapy transformed outcomes.
Then came:
Monoclonal antibodies.
Now emerging:
Immune engineering.
Future sequence:
Chemotherapy
→ Immunotherapy
→ Cell therapy
→ Intelligent oncology
Monoclonal Antibody Era
Targets:
- CD20
- CD19
- CD22
Impact:
Improved survival.
Targeted Therapy Era
Examples of mechanisms:
- BTK inhibition
- BCL-2 modulation
- PI3K targeting
Cellular Therapy Era
Potential areas:
- CAR-T
- NK-cell engineering
- Personalized immune oncology
7. Indian Lymphoma Market Beyond 2026
India’s lymphoma market forms part of the rapidly expanding hematology-oncology economy.
Key growth drivers:
Rising diagnosis
Hospital infrastructure growth
Private oncology expansion
Biosimilar penetration
Precision diagnostics
Insurance evolution
The Indian oncology ecosystem is increasingly moving toward integrated specialty care.
Figure 2 — Illustrative Indian NHL Market Outlook
| Year | Market Direction |
|---|---|
| 2026 | Expanding biologics access |
| 2030 | Precision adoption phase |
| 2035 | Molecular oncology scale-up |
| 2040 | Cell therapy integration |
Illustrative strategic outlook.
8. Global NHL Market Beyond 2026
The global lymphoma market may become one of the most technologically advanced oncology segments.
Major growth engines:
- Precision medicine
- Immunotherapy
- Cellular therapeutics
- Companion diagnostics
Expected structural transition:
Drug revenue
↓
Platform revenue
Future value pools:
Diagnostics
Data
Monitoring
Therapy
9. Precision Oncology and Indian Opportunities
India possesses unusual strengths:
- Pharmaceutical manufacturing
- Clinical expertise
- Biosimilar capabilities
- Cost-efficient innovation
Potential future domains:
Biomarker testing
Genomic services
Companion diagnostics
Cell therapy manufacturing
AI oncology platforms
10. Economic Segments Likely to Expand
Therapeutics
35%
Diagnostics
20%
Precision medicine
15%
Digital oncology
10%
Cell therapy
10%
Monitoring systems
10%
Illustrative future architecture.
11. Emerging Technologies That May Redefine NHL Care




Artificial Intelligence
Applications:
- Risk prediction
- Imaging interpretation
- Treatment support
Digital Pathology
Faster diagnostics.
Biomarkers
Personalized selection.
Continuous Monitoring
Longitudinal cancer management.
12. Access Challenges for India
Growth alone does not guarantee equity.
Critical barriers:
Geographic disparities
Cost pressure
Specialist shortages
Molecular testing access
Long-term affordability
Future leadership will depend not only on innovation—
but on democratization.
13. Pharmacology Perspective: The Coming Therapeutic Revolution
From a pharmacological viewpoint, NHL may become one of the clearest demonstrations of modern medicine’s transition:
Small molecules
→ Biologics
→ Cellular engineering
→ Adaptive therapy
The future lymphoma physician may increasingly function as:
Clinician
- Molecular interpreter
- Data strategist
14. Indian Research and Innovation Opportunities
Strategic areas:
- Indian genomic databases
- NHL biomarker repositories
- Real-world evidence platforms
- Cost-effective CAR-T models
- Academic–industry partnerships
India’s long-term opportunity may lie not merely in consuming oncology innovation—
but producing it.
15. NHL Beyond 2040: From Disease Management to Biological Control
The next era may shift questions.
Current:
“How do we treat lymphoma?”
Future:
“How do we predict transformation before symptoms emerge?”
Long-term possibilities:
- Ultra-early detection
- Adaptive treatment algorithms
- Prevention of relapse
- Immune ecosystem engineering
Conclusion
Non-Hodgkin lymphoma among Indians represents far more than a clinical diagnosis.
It is becoming a convergence point of:
Biology
Pharmacology
Data science
Precision medicine
Healthcare economics
and human resilience.
Beyond 2026, India’s lymphoma landscape may evolve from fragmented diagnosis and standardized treatment toward molecular classification, personalized intervention, and intelligent oncology systems.
The oncology economy of the future may not be built only on stronger drugs.
It may be built on better understanding.
And in lymphoma—
understanding biology may become the most powerful therapy of all.

